
Impact numbers
In this case study, we estimated the public health impact in the year following marketing authorisation of rimonabant in the UK, based on the England and Wales population data on obesity (http://www.noo.org.uk/data_sources).We chose this hypothetical scenario to assess whether impact numbers can be used in real-life regulatory activities such as for marketing authorisation approval or withdrawal.Note that this is an unlikely scenario in real life since we have not considered competing intervention for obesity, and the likely consumption (proportions and compliance) would also be much lower than those in clinical trials. The purpose here is only to demonstrate how the impact numbers may be used.
We ran impact number analysis for year 2006 when rimonabant just came on the market, where evidence of benefits and risks were only from the four RIO trials. The data have been summarised in MCDA (Deterministic) section, and the stochastic parameters accounting for the uncertainty in the data are described in the Probabilistic Simulation section.
We investigated two impact numbers here: the number of events prevented in the population (NEPP) and the population impact number of eliminating a risk factor over time t (PIN-ER-t). The use of these two impact numbers along with exposure impact number (EIN) was first published in 2011 (Verma, 2011).Figure 1 and Figure 2 below show PIN-ER-1 and NEPP for benefit criteria, respectively. Likewise, Figure 3 and Figure 4 show PIN-ER-1 and NEPP for risk criteria, respectively.
Figure 1Population impact number of eliminating a risk factor over one year (PIN-ER-1) and 95% confidence intervals for benefits in 2006 in England and Wales population
{kind=link}
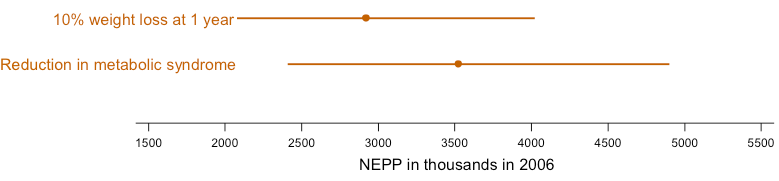
Figure 2 Number of events prevented in population (NEPP) and 95% confidence intervals for benefits in 2006 in England and Wales population
{kind=link}
Based on the data and assumptions we made in this case study, for example, we would observe a median of 1,625,149 people who achieved a 10% weight loss in one year due to rimonabant, with a 95% confidence interval between 1,298,561 and 1,989,220 people (PIN-ER-1 in Figure 1).By introducing rimonabant into the population (under the current assumptions), a total of 2,917,808 people (95% CI from 2,076,566 to 4,021,742)may benefit from a 10% weight loss within one year (NEPP in Figure 2). Similar interpretations can be used for other criteria in the model.
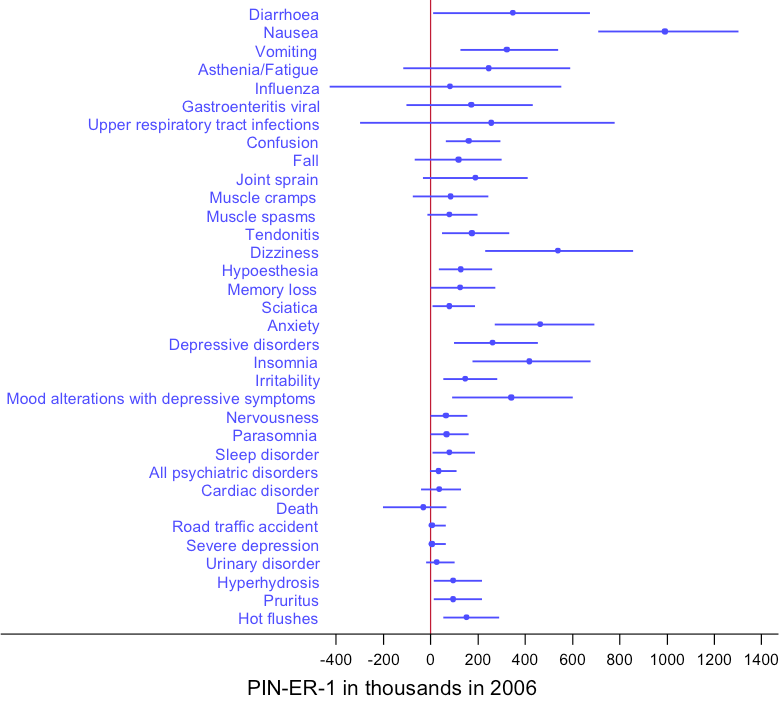
Figure 3Population impact number of eliminating a risk factor over one year (PIN-ER-1) and 95% confidence intervals for risks in 2006 in England and Wales population
{kind=link}
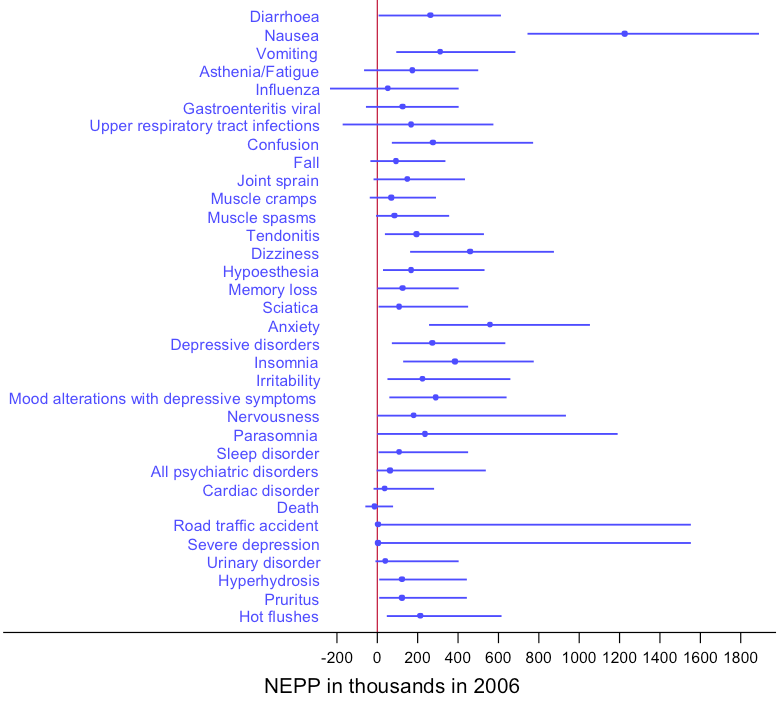
Figure 4 Number of events prevented in population and 95% confidence intervals for risks in 2006 in England and Wales population
{kind=link}
The applications of impact numbers are unique to the decision problems. The questions that assessors asked would drive how the impact numbers are interpreted. Therefore, it is important to set clear objectives upfront. We struggled with interpreting our results in this case study because we tried to make the applications of impact numbers as broad as possible, where the strengths lie in the specifics of the decision problems. We encourage readers to properly think through the benefit-risk assessment process and the specific objectives and decisions to be made when using impact numbers. Since impact numbers are calculated criterion-wise, it may be difficult to establish the overall benefit-risk balance of an intervention (e.g. rimonabant) especially when there are multiple criteria involved. We further investigated simple methods to integrate one benefit and one risk criteria to at least assess the benefit-risk balance of rimonabant on the most important drivers (see Benefit-Risk Ratio and Net Clinical Benefit sections). Further work is needed to integrate multiple impact numbers on the benefit and risk criteria to support decision-making.