
Sarac's Benefit-Risk Assessment Method (SBRAM)
We also tested Sarac's Benefit-Risk Assessment Method (SBRAM). We demonstrated here the weighting and scoring process in SBRAM, presenting the results for the indication of acute exacerbations of chronic bronchitis (AECB). More detailed descriptions and results are available in the Telithromycin Case Study Report.
It is expected that the benefit-risk balance for telithromycin will be positive for all four indications and that the market authorisation can be kept without restriction. All benefit and risk criteria can be seen in table 3. Criteria are weighted on a scale of 1, 2 and 3 to represent increasing importance to the overall assessment (i.e. 1 = lowest importance, 3 = highest importance), the weighting is considered the same for all indications.
Table 3: Weighting of benefit and risk criteria
| Criterion | Justification | Weight |
|---|---|---|
| Cure | This is primary endpoint for all antibiotics. | 3 |
| Syncope | There have been post-marketing adverse event reports of transient loss of consciousness including some cases associated with vagal syndrome. | 2 |
| Visual | Visual disturbances particularly in slowing the ability to accommodate and the ability to release accommodation. Visual disturbances include blurred vision, difficulty focusing, and diplopia. Most events are mild to moderate; however, severe cases have been reported. | 1 |
| Cardiac | Telithromycin has the potential to prolong the QTc interval of the electrocardiogram in some patients, which may lead to an increased risk of ventricular arrhythmias, including torsades de pointes. Thus, telithromycin should be avoided in patients with congenital prolongation of the QTc interval, and in patients with on-going proarrhythmic conditions such as uncorrected hypokalaemia or hypomagnesaemia, clinically significant bradycardia, and in patients receiving Class IA (e.g., quinidine and procainamide) or Class III (e.g., dofetilide) antiarrhythmic agents. Cases of torsades de pointes have been reported post-marketing with telithromycin. In clinical trials, no cardiovascular morbidity or mortality attributable to QTc prolongation occurred with telithromycin treatment in 4780 patients in clinical trials, including 204 patients having a prolonged QTc at baseline. | 2 |
| SAE | There exist several other antibiotics for the same indications. Therefore any tendency showing an unfavourable number of SAEs for telithromycin will be highly concerning. | 3 |
| Hepatic | Acute hepatic failure and severe liver injury, in some cases fatal, have been reported in patients treated with telithromycin. These hepatic reactions included fulminant hepatitis and hepatic necrosis leading to liver transplant, and were observed during or immediately after treatment. In some of these cases, liver injury progressed rapidly and occurred after administration of a few doses of telithromycin. | 3 |
Scoring is based on the probability of the drug of interest outperforms the comparator i.e. P(XDrug > XComparator)≥ α, where α = 2/3. The value of α can be changed to represent a lower or higher proportion as long as α lies within [0.5, 1]. For scoring of telithromycin data, we used the default α = 2/3. The evaluation of uncertainty and evidence is done qualitatively where the criteria with borderline scores are changed to interval scores. The weight and scores are then multiplied together, yield the weighted score (Table 4).
Table 4: Weighted scores of the SBRAM method, for all criteria in all four indications for telithromycin
| Criterion | Weight | Score | Weighted | Score | |||||
|---|---|---|---|---|---|---|---|---|---|
| CAP | ABS | AECB | TP | CAP | ABS | AECB | TP | ||
| Cure | 3 | +1 | 1 | 0 | 0 | +3 | 3 | 0 | 0 |
| 3 | - | - | 0-1 | - | - | - | 0-2 | - | |
| Syncope | 2 | 0-1 | 0-1 | -1 | 0 | 0-2 | 0-2 | -2 | 0 |
| Visual | 1 | -1-0 | -1 | -1 | -1 | -1-0 | -1 | -1 | -1 |
| Cardiac | 2 | 0-1 | 0-1 | 0-1 | 0 | 0-2 | 0-2 | 0-1 | 0 |
| SAE | 3 | 1 | -1-0 | -1 | 0 | 3 | -3-0 | -3 | 0 |
| Hepatic | 3 | 1 | -1 | 0 | +1 | 3 | -3 | 0 | +3 |
| TEAE | 1 | 1 | -1 | -1 | -1 | 1 | -1 | -1 | -1 |
SBRAM results for the indication of acute exacerbation of chronic bronchitis (AECB)
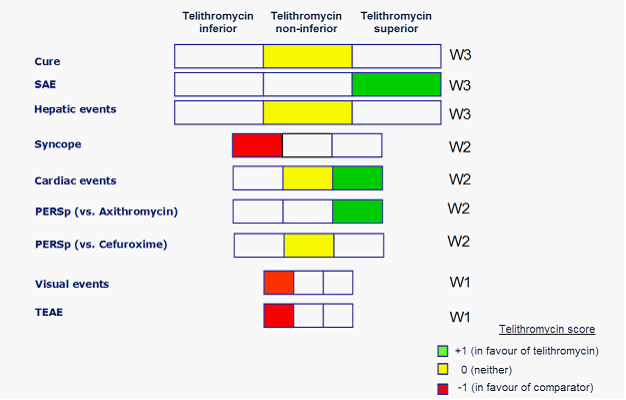
The overall benefit-risk for telithromycin versus grouped comparators in SBRAM is presented visually as a tornado-like diagram, shown in figure 20. The high important benefit criteria "cure" was not in favour of neither telithromycin nor comparators. For the high important risk criteria, "SAEs" are in favour for telithromycin, while there are no tendencies towards either drug or comparator for the criteria "Hepatic AEs". This is also the case for the risk criteria "Cardiac AEs", while the other medium important risk criteria are in favour for comparator. The two low important risk criteria are also in favour for comparator. Based on these results the benefit-risk balance for telithromycin for the indication AECB is considered to be negative. However in the indication of AECB there is data from a phase IV trial on penicillin- or erythromycin-resistant S pneumoniae (PERSp) at TOC (test of cure). For these criteria, telithromycin versus azithromycin shows a favour for telithromycin, whereas telithromycin versus cefuroxime shows no difference between them.
Figure 20: SBRAM tornado-like diagram visualising overall benefit-risk of telithromycin versus grouped comparators for the indication AECB.
{kind=link}
SBRAM also uses a scoring chart to visualise the "position" of an event for a drug of interest versus a comparator, set against the scores -1, 0 and +1. Figure 21 shows the (enlarged) scoring chart for the AECB benefit criteria "cure" using the data pooled from phase III comparative and phase IV studies. A scoring chart may contain more than one criteria.
Figure 21: A scoring chart for criterion cure for the indication of AECB, showing that 413 people were cured in the telithromycin arm and 416 people were cured in the comparator arm
{kind=link}
Comments on SBRAM
Data analysis (scoring) methodology for discrete data uses data direct (trial size N and number of events x) and the method cannot accommodate input from meta-analysis. The scoring for discrete data is based on P(XDrug > XComparator) ≥ α, α = 2/3. An approximation to the principle of scoring could be developed which uses the probability, p of an event for drug and comparator and the confidence interval for the probabilities. In the SBRAM a scoring approach for continuous data has been described based on P(XDrug > XComparator) ≥ α, α = 2/3. P(XDrug > XComparator) and may be calculated from the difference distribution, simply as the area under the curve from 0 to infinity. In the telithromycin analysis only two options are identified, due to limitations in available data. However if several options have to be assessed with the same set of benefit and risk criteria and weighting, the SBRAM compares two options at a time. In connection to the decision whether to put restriction on one or more of the indications, the benefit criteria (cure) could, for at least the indication CAP, be split up into (1) cure - general population and (2) cure - high antibiotic resistance population.