
Multi-criteria decision analysis (MCDA)
The MCDA is based on the problem described under PrOACT-URL Framework. We provide a high-level overview of the analysis, and show some results of the benefit-risk analysis of telithromycin versus comparators for the AECB indication. More detailed descriptions and results are available in the Telithromycin Case Study Report.
Value tree
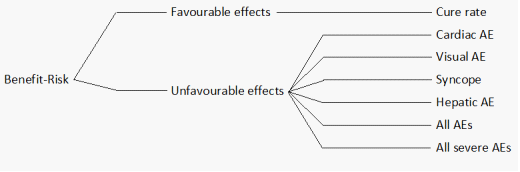
An overview of benefit and risk criteria used in the model is shown in the value tree in figure 3.
Figure 3: Value tree for the MCDA assessment of telithromycin versus grouped comparators, for each of the four indications AECB, TP, ABS and CAP.
{kind=link}
Preference scores
Value function for each criterion was defined. All preference scores between the two options were established on a fixed scale based on a linear preference scoring. The range of preference scale was anchored according to clinical importance based on an in-group physician opinion. Data suggested that difference in efficacies between treatments was small and we were more interested in difference in risk, so the margin in benefit was fixed at 0 and 100%, whereas risk was fixed at 0 and 10%.
Weighting
Ideally, the weighting requires a decision conference between stakeholders to achieve an agreed weightings and tread-offs, however for this analysis this was not feasible. Weightings on criteria were assigned by a physician and benefit¨Crisk weightings were based on the clinical context. Complex weightings between risk criteria were assigned using the Measuring Attractiveness by a Categorical Based Evaluation Technique (MACBETH) approach in HiView3. This was done independently for each indication assessed (AECB, TP, ABS, and CAP).
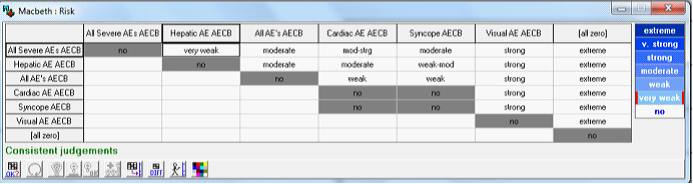
For the AECB indication, the weights for the analysis of telithromycin versus grouped comparators are shown in table 2. The benefit criterion was given a higher weighting due to concerns with an existing antibiotics resistance in AECB. The weighting of risk criteria of was done among the case study team members using MACBETH, see figure 4.
Table 2: Criteria weighting AECB
| Criteria | Weight | Sub Criteria | Weight |
|---|---|---|---|
| Benefit | 0.70 | Cure rate | 1.00 |
| Risk | 0.30 | Cardiac AE | 0.16 |
| Visual AE | 0.11 | ||
| Syncope | 0.16 | ||
| Hepatic AE | 0.20 | ||
| Severe Adverse events | 0.20 | ||
| All adverse events | 0.17 |
Figure 4: Macbeth approach for weighting of risk criteria in the indication AECB
{kind=link}
Benefit-risk results
The results of each MDCA model was analysed based on overall benefit-risk value, the contribution of each criteria to the overall benefit-risk value and from the difference display, showing the weighted difference between the two alternatives for each criterion. Furthermore, the sensitivity analysis of the robustness of the model to changes in assigned criteria weights was made for each model.
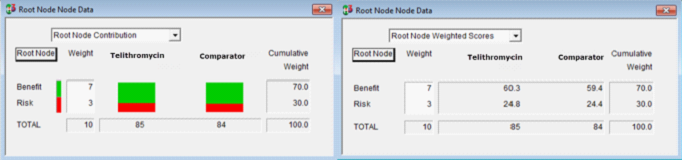
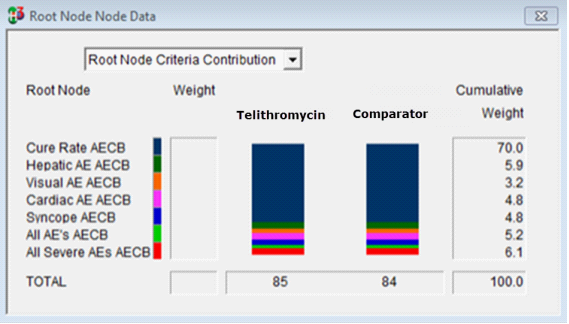
As an example, tor the treatment of AECB, the overall results showed telithromycin would be a more preferable choice by a small margin. There was a small difference in cure rate with telithromycin (see figure 5) as well as lower combined score in adverse events. Figure 6 shows criteria contribution to the overall benefit-risk scores. The difference display (Figure 7) it shows that telithromycin achieved a higher weighted score with cure rate, incidence of cardiac AE and hepatic AE, as well as overall adverse event rate.
Figure 5: Overall results from MDCA analysis of telithromycin versus grouped comparator for treatment of AECB (Screenshot from software HiView3)
{kind=link}
Figure 6: Contribution from each criteria of the MDCA analysis of AECB (screenshot form HiView3)
{kind=link}
Figure 7: Difference diagram from AECB analysis shows the weighted difference between telithromycin versus grouped comparator for each criterion (screenshot from HiView3). Green bars indicate a weighted difference in favour to telithromycin and red in disfavour.
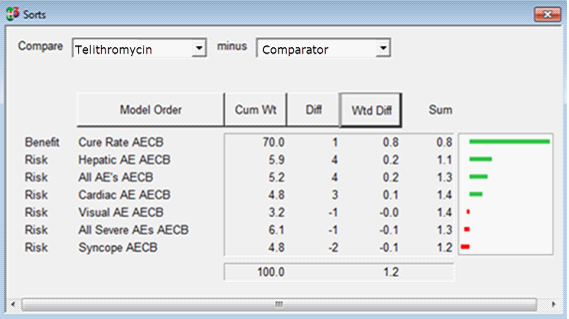{kind=link}
Sensitivity analysis
Sensitivity analysis was carried out to assess whether the MCDA results could be influenced by changes in weightings assigned in assessment of telitromycin versus grouped comparators for treatment of AECB. The model was found to be very robust to change in criteria weights (see figure 8 and figure 9 ), only large increase in the weight of the criteria visual AE, syncope and all severe AE change the overall benefit-risk balance to be in favour of grouped comparators over telithromycin.
Figure 8: Sensitivity testing, effect of changing the weight on benefit and risk from the assigned 70-30 split in the AECB analysis (Screenshot from HiView3). On the horizontal axis is the benefit category weight and on the vertical axis the overall benefit-risk value.
{kind=link}
Figure 9: Sensitivity analysis on each risk criteria of the AECB model (screenshot from HiView3), weight on horizontal axis and overall benefit-risk value on vertical axis.
{kind=link}