
Net Clinical Benefit (NCB)
Data from CPRD-link database are used to estimate as accurately as possible the individual risk of bleeding and stroke in patients with atrial fibrillation (AF) treated with warfarin. Furthermore we explore characteristics that influence the individual benefit-risk balance.
Method
Data source:
Data was extracted from Clinical Practice Research Datalink (CPRD), in addition data from Hospital Episode Statistics (HES).
The study design was a retrospective cohort. The start of follow-up was 1st January 1990 the start of CPRD or HES data collection of each patient, whichever came last. End of follow-up was the earliest end of data collection for each patient in DCPD or HES. Patients were censored 6 months after the data of the last warfarin perception.
The cohort of warfarin users included patients aged >=18 years with a documented record of AF. The index data was the first warfarin prescription issued at least 12 months after start of data collection. Patients with a record of rheumatic valve disease or patients with valvular repair/replacement were excluded.
Outcomes (criteria):
Benefit- Ischaemic stroke (recorded in HES)
- Transient ischaemic attack (recorded in CPRD)
Risk
- Haemorrhagic stroke (recorded in HES)
- Major bleed (recorded in HES). Major bleed was defined as symptomatic bleeding in a critical area or organ (excluding intracranial), such as intra-spinal, intraocular, retroperitoneal, gastrointestinal, intra-articular or pericardial, or intramuscular with compartment syndrome
Individual benefit-risk balance
Attributable risk and benefit for each individual was calculated.19 First the cumulative incidence (CI) of an event for each set of patients characteristics using the survivor function in the cox-proportional hazard regression model. This is done to allow calculation of an individual's probability of an outcome. The second step is to obtain an estimate on the likely effects. Here it is assumed that there relative rate (RR) found in RCTs is an unbiased estimate of the drug effect and is expected to be consistent across the population. RR is used to estimate the underlying (unexposed) event probability. The attributable risk is the difference between the exposed and unexposed event probabilities (see table 19 for schematic representation)
Table 19: Schematic representation of Attributable risk
| RR = cumulative incidence exposed/cumulative incidence unexposed, where RR extracted from the literature, cumulative incidence exposed is estimated from database with cox-proportional hazard model Attributable risk (benefit) = cumulative incidence exposed - cumulative incidence unexposed |
|---|
RR was based on data from RCT identified in the literature. The RR used in this model can be seen in table 20
Table 20: Relative risk (RR) used in model
| Outcome | Relative rate | Source |
|---|---|---|
TIA
| 0.45 |
*Approximation from OR |
|
Ischaemic stroke
| 0.28 |
Meta-regression data from 5 RCT |
|
Haemorrhagic stroke
| 2.38 |
*Approximation from OR |
|
Major Bleed
| 1.23 |
Meta-regression data from 5 RCT |
|
| *Due to low incidence rates for stroke, TIA and haemorrhage in both unexposed and warfarin exposed patient it is assumed that RR can be approximated from OR (odds rate) | ||
The ischaemic stroke and TIA prevented with warfarin and the additional haemorrhage stroke events and major bleed event with warfarin compared the unexposed were calculated by taken the average difference between cumulative incidence exposed and cumulative incidence unexposed per 1000 patients. The results were stratified for risk of ischaemic stroke based on the CHA2DS2-VASc and for risk of bleeding according to HAS-BLED
- CHA2DS2-VASc : (congestive heart failure, hypertension, age > 75, diabetes mellitus, stroke, vascular disease, age 65-64 and female gender)
- HAS-BLED: (hypertension, abnormal liver/kidney function, stroke, bleed, labile INR, age > 65, drugs/alcohol intake)
Net benefit was calculated based on following:
- Net benefit = (Prevention of ischaemic stroke + Prevention of TIA*0.84) - (Occurrence of Haemorrhagic stroke*1.7 - Occurrence of Major bleed*0.91)
The weight was chosen on the basis of the 1-year mortality of the outcome compared to the mortality of ischaemic stroke.
Finally three groups were defined unfavourable (net benefit < 0.5) favourable (net benefit 0.5-1.5) and very favourable (net benefit > 1.5). The limits were defined based on the variation of the net benefit across the population. Net benefit around average was considered to be favourable, patients that were below or above this average range were considered to be respectively unfavourable or very favourable, quartiles for the net benefit is shown in table 21. We used logistic regression to find characteristics that were associated with having an unfavourable net benefit, because for these patients warfarin treatment is not necessarily the best choice.
Table 21: Range of quantiles of net benefit
| Quantile | Estimate |
|---|---|
| 100% | 1675.7 |
| 99% | 10.1 |
| 95% | 4.2 |
| 90% | 2.5 |
| 75%Q3 | 1.5 |
| 50%Median | 1.0 |
| 25%Q1 | 0.6 |
| 10% | 0.2 |
| 5% | -0.7 |
| 1% | -11.8 |
| 0%Min | -404.5 |
Results
The study cohort consisted of 33,772 patient with atrial fibrillation exposed to warfarin, mean age 74.5 (SD 11.3) baseline characteristics are shown in table 22.
Table 22: Baseline characteristics of cohort population(Warfarin users N = 33772)
| Characteristic | Category | N | % |
|---|---|---|---|
| Gender (male) | Male | 17485 | 51.8 |
| |
|
|
|
Age
| <65 |
5923 |
17.5 |
|
| 65-74 |
9053 |
26.8 |
|
| 75-84 |
12611 |
37.3 |
|
| >85 |
6185 |
18.3 |
|
Social economic status
| 20% (most deprived) |
7559 |
22.4 |
|
| 21-40% |
8614 |
25.5 |
|
| 41-60% |
7061 |
20.9 |
|
| 61-80% |
6011 |
17.8 |
|
| 81-100% (least deprived) |
4527 |
13.4 |
|
Smoking status
| Current smoker |
23907 |
70.8 |
|
| Non-smoker |
4609 |
13.6 |
|
| Ex-smoker |
3569 |
10.6 |
|
| Unknown |
1687 |
5.0 |
|
Body mass index (kg/m2)
| Underweight (<20) |
1138 |
3.4 |
|
| Normal (20-<25) |
7970 |
23.6 |
|
| Overweight (25-<30) |
11974 |
35.5 |
|
| Obese (>=30) |
8612 |
25.5 |
|
| Unknown |
4078 |
12.1 |
|
CHA2DS2-VASc
| High |
6172 |
18.3 |
|
| Moderate |
7497 |
22.2 |
|
| Low |
20103 |
59.5 |
|
HAS-BLED
| High |
3192 |
9.5 |
|
| Moderate |
3351 |
9.9 |
|
| Low |
27229 |
80.6 |
|
Prescribing in the 6 months before index date
| Antiplatelets |
14673 |
43.4 |
|
| Antidepressants |
3266 |
9.7 |
|
| Antidiabetics |
2183 |
6.5 |
|
| NSAIDS (excl. aspirin) |
5743 |
17.0 |
|
| Corticosteroids (rectal or oral) |
2699 |
8.0 |
|
| Hypnotics |
2768 |
8.2 |
|
| Medicines that have interactions with warfarin |
20473 |
60.6 |
|
Diagnoses ever before index date
| Liver failure |
179 |
0.5 |
|
| Anemia |
22423 |
66.4 |
|
| Congestive heart failure |
1298 |
3.8 |
|
| Coronary heart disease |
4899 |
14.5 |
|
| Diabetes mellitus |
9362 |
27.7 |
|
| Alcohol and drug abuse |
4088 |
12.1 |
|
| Falls |
744 |
2.2 |
|
| Hypercholesterolemia |
3741 |
11.1 |
|
| Hypertension |
5083 |
15.1 |
|
| Major bleed |
16170 |
47.9 |
|
| Cancer |
1861 |
5.5 |
|
| Minor bleed |
8473 |
25.1 |
|
| Proteinuria |
4361 |
12.9 |
|
| Renal insufficiency |
348 |
1.0 |
|
| Stroke ischaemic |
792 |
2.3 |
|
| Stroke haemorhagic |
29167 |
86.4 |
|
| Stroke unspecificed |
898 |
2.7 |
|
| Thrombocytopenia |
129 |
0.4 |
|
| TIA |
2308 |
6.8 |
|
| Vascular disease |
110 |
0.3 |
|
| Deep Venous Thrombosis |
2706 |
8.0 |
|
| Pulmonary embolism |
4220 |
12.5 |
|
Net benefit-harm stratified by risk of stroke (CHA2DS2-VAS2) and risk of bleeding (HAS-BLED) are shown in table 23, and by baseline risk of stroke in table 24.
Table 23: Potential number of prevented ischaemic strokes, transient ischaemic attacks, and number of excess cases of haemorrhagic stroke, major bleed stratified by baseline risk for stroke (according to CHA2DS2-VASc) and bleeding (according to HAS-BLED)
| Baseline risk stroke (CHA2DS2-VASc) | Baseline risk bleed(HAS-BLED) | Benefits (no. of cases prevented per 1000 patients) | Risks (excess no. of cases per 1000 patients) | Benefit - Harm | ||
|---|---|---|---|---|---|---|
| Ischaemic stroke(reported in HES) | Transient ischaemic attack (reported in CPRD) | Haemorrhagic stroke (reported in HES) | Major bleed (reported in HES) | |||
High
| High |
112 |
47 |
10 |
54 |
+85
| |
Moderate
| High |
119 |
46 |
20 |
46 |
+82
| |
Low
| High |
78 |
0 |
0 |
78 |
+7
| |
High
| Moderate |
93 |
57 |
14 |
52 |
+70
| |
Moderate
| Moderate |
66 |
45 |
9 |
50 |
+43
| |
Low
| Moderate |
73 |
33 |
8 |
54 |
+38
| |
High
| Low |
71 |
28 |
8 |
63 |
+24
| |
Moderate
| Low |
52 |
24 |
8 |
55 |
+8
| |
Low
| Low |
46 |
27 |
8 |
45 |
+15
| |
| *Events were weight by their 1-year mortality compared to ischaemic stroke; transient ischaemic attack (0.84), haemorrhagic stroke (1.70), major bleed (0.91) | ||||||
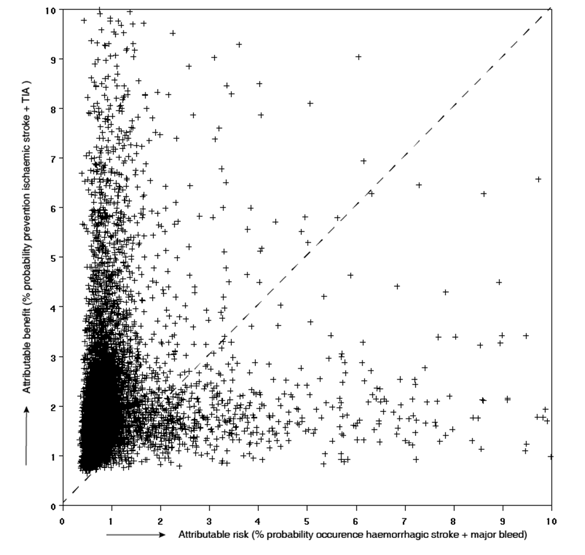
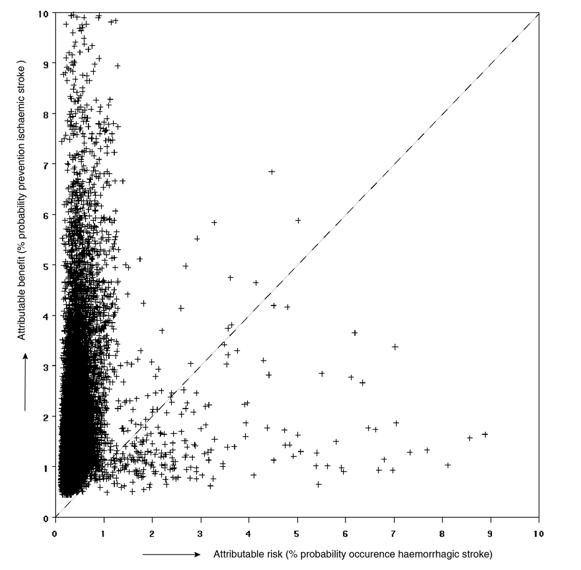
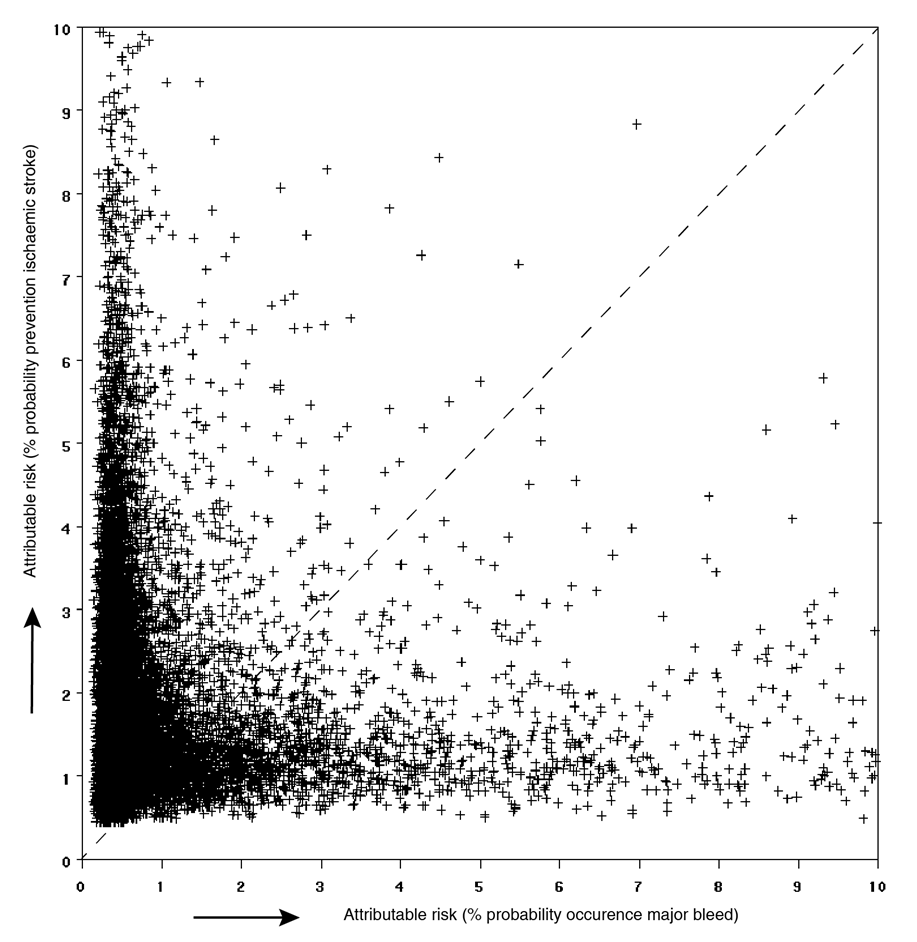
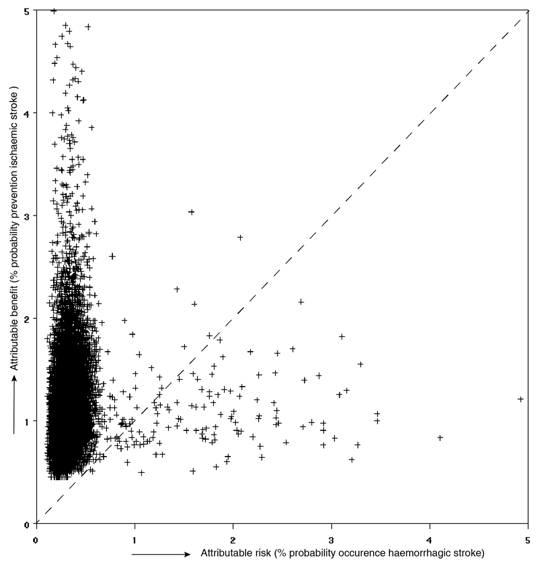
The benefit-risk plane shows attributable benefit and attributable risk represented in the y-axis and the x-axis respectively. For this representation only one benefit criteria and one risk criteria can be represented, forFigure 23 the benefit criteria ischaemic stroke and TIA are group and the risk criteria haemorrhagic stroke and major bleed are grouped. Figure 24 and figure 25 show ischaemic stroke versus haemorrhagic stroke and versus major bleed, respectively.
Figure 23: Potential risk (occurrence of haemorrhagic stroke + major bleed) versus potential benefit (prevention of ischaemic stroke + TIA)
{kind=link}
Figure 24: Potential risk (occurrence of haemorrhagic stroke) versus potential benefit (prevention of ischaemic stroke) in four years
{kind=link}
Figure 25: Potential risk (occurrence of major bleed) versus potential benefit (prevention of ischaemic stroke) in four years.
{kind=link}
In Figure 26 and figure 27, the attributable benefit of ischaemic stroke is plotted versus the attributable risk of haemorrhagic stroke, stratified for baseline risk of stroke and bleed.
Figure 26: Potential risk (haemorrhagic stroke) versus potential benefit (ischaemic stroke) in four years due to treatment with warfarin versus no treatment for prevention of stroke in patient with atrial fibrillation having high risk of stroke (CHADSVASC >= 2) and high risk of bleed (HADBLED >= 2).
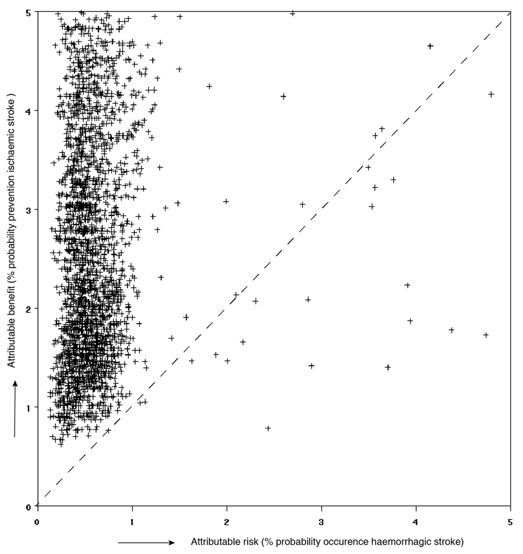{kind=link}
Figure 27: Potential risk (haemorrhagic stroke) versus potential benefit (ischaemic stroke) in four years due to treatment with warfarin versus no treatment for prevention of stroke in patient with atrial fibrillation having low risk of stroke (CHADSVASC<=2) and low risk of bleed (HADBLED <= 2)
{kind=link}
The mean net benefit was 1.17 (SD 16.0) ischaemic stroke cases or equivalent prevented. A total of 7036 (20.8%) patients were classified as having an unfavourable benefit-risk balance and 7950 (23.54%) as having a very favourable benefit-risk balance. The rest of the patients had a favourable net benefit. Table 25: Characteristics associated with a less favourable (<0.5) net benefit.Table 25lists the characteristics that were significantly associated with aunfavourable benefit-risk balance
Table 25: Characteristics associated with a less favourable (<0.5) net benefit.
| Characteristic | Odds ratio (95% CI) | Unfavourable | Very favourable | |
|---|---|---|---|---|
| Prescriptions ( 6 months before index date) | ||||
Antiplatelet agents | No | Reference | 4013 (50.8) | 3886 (49.2) | |
| Yes | 1.38 (1.21-1.57) | 3937 (55.6) | 3150 (44.5) | |
Anti-diabetic drugs | No | Reference | 6747 (49.11) | 6991 (50.9) | |
| Yes | 1.70 (1.25-2.30) | 289 (23.16) | 959 (76.8) | |
Corticosteroids | No | Reference | 6220 (45.7) | 7397 (54.3) | |
| Yes | 1.99 (1.60-2.46) | 816 (59.6) | 553 (40.4) | |
Hypnotics | No | Reference | 6522 (48.2) | 7011 (51.8) | |
| Yes | 0.68 (0.57-0.83) | 514 (35.4) | 939 (64.6) | |
NSAID\'s | No | Reference | 6063 (50.0) | 6064 (50.0) | |
| Yes | 0.27 (0.23-0.31) | 973 (34.0) | 1886 (66.0) | |
| Medicines that have interactions with warfarin* | No | Reference | 2393 (46.7) | 2735 (53.3) |
| Yes | 1.32 (1.16-1.52) | 4643 (47.1) | 5215 (52.9) | |
| Comorbidities (ever before index date) | ||||
Anaemia | No | Reference | 6828 (47.9) | 7428 (52.1) | |
| Yes | 0.30 (0.22-0.40) | 208 (28.5) | 522 (71.5) | |
Congestive heart failure | No | Reference | 5713 (46.2) | 6666(53.9) | |
| Yes | 2.67 (2.27-3.14) | 1323 (50.8) | 1284 (49.3) | |
Coronary heart disease | No | Reference | 5427 (54.5) | 4538 (45.5) | |
| Yes | 0.52 (0.45-0.61) | 1609 (32.1) | 3412 (68.0) | |
Diabetes Mellitus | No | Reference | 6585 (52.1) | 6066 (48.0) | |
| Yes | 0.06 (0.05-0.06) | 451 (19.3) | 1884 (80.7) | |
Falls | No | Reference | 5930 (45.8) | 7029 (54.2) | |
| Yes | 2.14 (1.79-2.57) | 1106 (54.6) | 921 (45.4) | |
Hypertension | No | Reference | 3746 (53.5) | 3250 (46.5) | |
| Yes | 0.41 (0.36-0.46) | 3290 (41.2) | 4700 (58.8) | |
Ischaemic stroke | No | Reference | 6988 (48.4) | 7451 (51.6) | |
| Yes | 0.20 (0.12-0.33) | 48 (8.78) | 499 (91.22) | |
Cancer | No | Reference | 4526 (42.3) | 6172 (57.7) | |
| Yes | 2.51 (2.19-2.88) | 2510 (58.5) | 1778 (41.5) | |
Minor bleed | No | Reference | 5739 (45.0) | 7014 (55.0) | |
| Yes | 2.68 (2.19-2.88) | 1297 (58.1) | 936 (41.9) | |
Renal insufficiency | No | Reference | 6766 (46.7) | 7729 (53.3) | |
| Yes | 3.30 (2.37-4.60) | 270 (55.0) | 221 (45.0) | |
TIA | No | Reference | 6617 (49.5) | 6739 (50.5) | |
| Yes | 0.52 (0.43-0.64) | 419 (25.7) | 1211 (74.3) | |
Vascular disease | No | Reference | 6534 (52.9) | 5829 (47.2) | |
| Yes | 0.16 (0.13-0.19) | 502 (19.1) | 2121 (80.9) | |
Table 26 shows the actual numbers of warfarin users identified within CPRD in different categories of favourability; from the most favourable category in which a patient has the benefits, but not the adverse events to the patients who do not have the benefits, but do have the adverse events.
Table 26: Absolute number of events in warfarin users in different categories of favourability
| No Haemorrhagic Stroke | Haemorrhagic Stroke | ||||
|---|---|---|---|---|---|
| No Major Bleed | Major Bleed | No Major Bleed | Major Bleed | ||
| No Ischemic Stroke | No TIA | 23563 | 1235 | 209 | 11 |
| TIA | 323 | 33 | 7 | 1 | |
| Ischemic Stroke | No TIA | 296 | 35 | 14 | 1 |
| TIA | 31 | 4 | 1 | 0 | |